- Ben Haresign
- 20 Jun, 2026
- Access
- 9 min read
Why can’t I get a GP appointment? Follow the money
General practice · Access · Funding
Why Can’t I Get a GP Appointment? Follow the Money
General practice is delivering millions of appointments, answering tens of millions of calls and managing rapidly growing online demand. Yet many patients still find it difficult to access care. The problem is not that practices have stopped working. It is that demand has expanded faster than the capacity funded to meet it.

The blunt answer
England has built a system in which general practice is expected to operate as the NHS switchboard, triage hub, prevention engine and community front door — without consistently funding the front door as though it were the front door.
General practice is not doing less
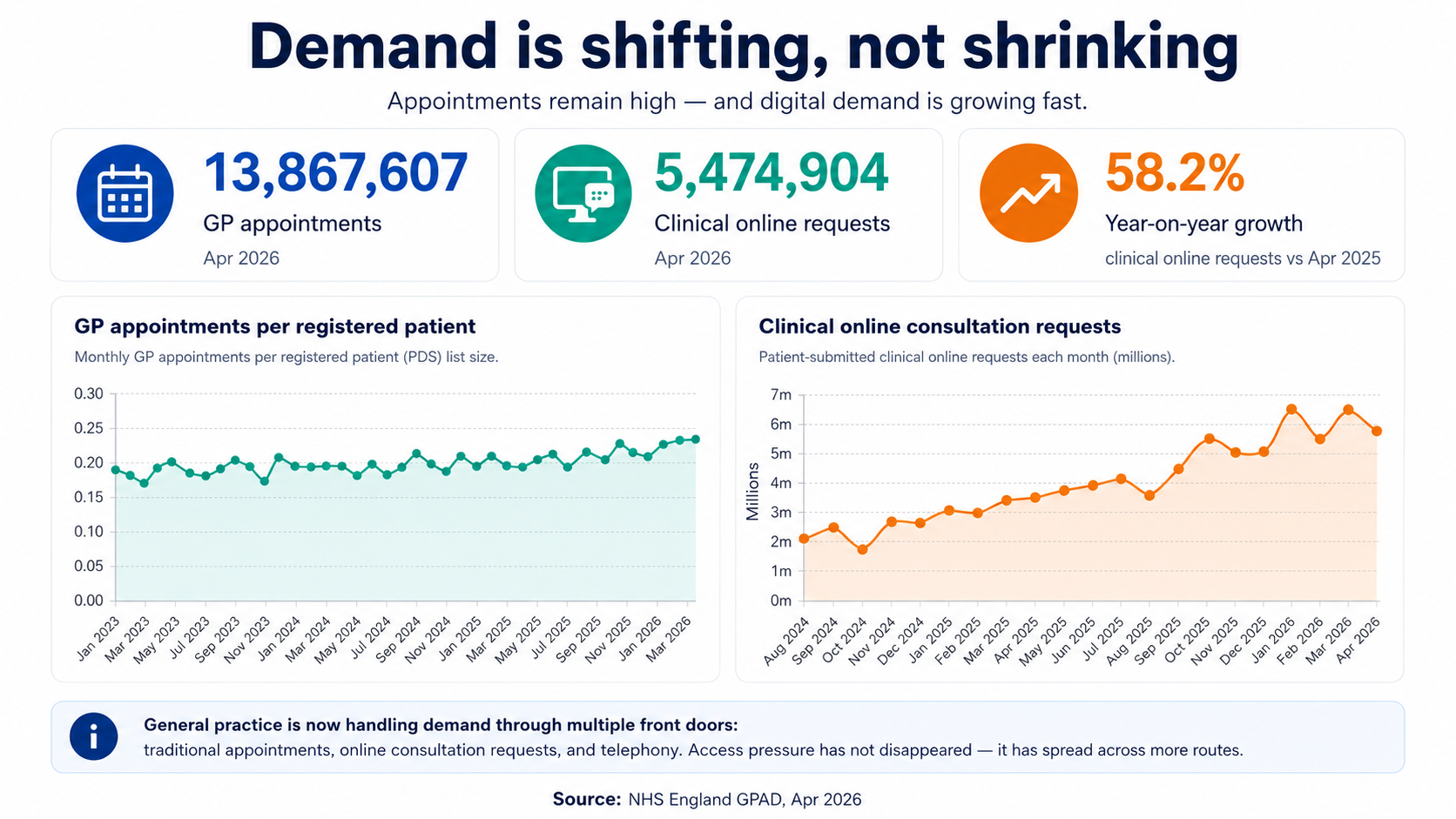
In April 2026, practices in England recorded 13,867,607 GP-delivered appointments. That was 6.1% higher than a year earlier. Across the latest completed 12-month period, practices continued to deliver hundreds of millions of appointments through GPs, nurses, healthcare assistants, pharmacists and other members of the primary care team.1
The national data does not describe a service sitting idle. It describes one operating at sustained high volume, month after month, while also taking on work that may not appear in a traditional appointment count.
Every clinical request must be received, reviewed and directed. Some become face-to-face consultations. Others become telephone calls, prescriptions, investigations, referrals, messages, advice or urgent escalation. The absence of a booked appointment does not necessarily mean that no work took place.
National totals are important, but they can also hide the local reality. Demand is not distributed evenly. Practices serving older populations, patients with greater deprivation, higher levels of long-term illness or rapidly growing housing developments may face substantially greater workload than the national average suggests.
Demand has not disappeared. It has multiplied.
Telephone appointments were once the main alternative to a face-to-face consultation. General practice now receives demand through several front doors at once:
Telephone
Calls, callbacks, messages and telephone consultations.
Online requests
Clinical forms that must be reviewed, prioritised and answered.
Appointments
Care delivered by GPs and the wider multidisciplinary team.
Administrative work
Results, prescriptions, referrals, letters, records and reports.
In April 2026, practices recorded 5,474,904 patient-submitted clinical online requests. That was approximately 58.2% more than in April 2025.1
Online access can make it easier for patients to contact their practice, but it does not remove the clinical work. It changes how the work arrives. Every request still needs somebody to read it, assess risk, check the record, decide what response is required and complete the resulting action.
Digital access can therefore reveal demand that was previously suppressed by busy telephone lines. It may improve convenience while simultaneously increasing the volume of work reaching the practice.
Why the telephone experience can still feel so difficult
For many patients, the pressure becomes visible at 8am. That makes the telephone system an easy target, but the queue is usually a symptom of the wider capacity problem rather than its cause.
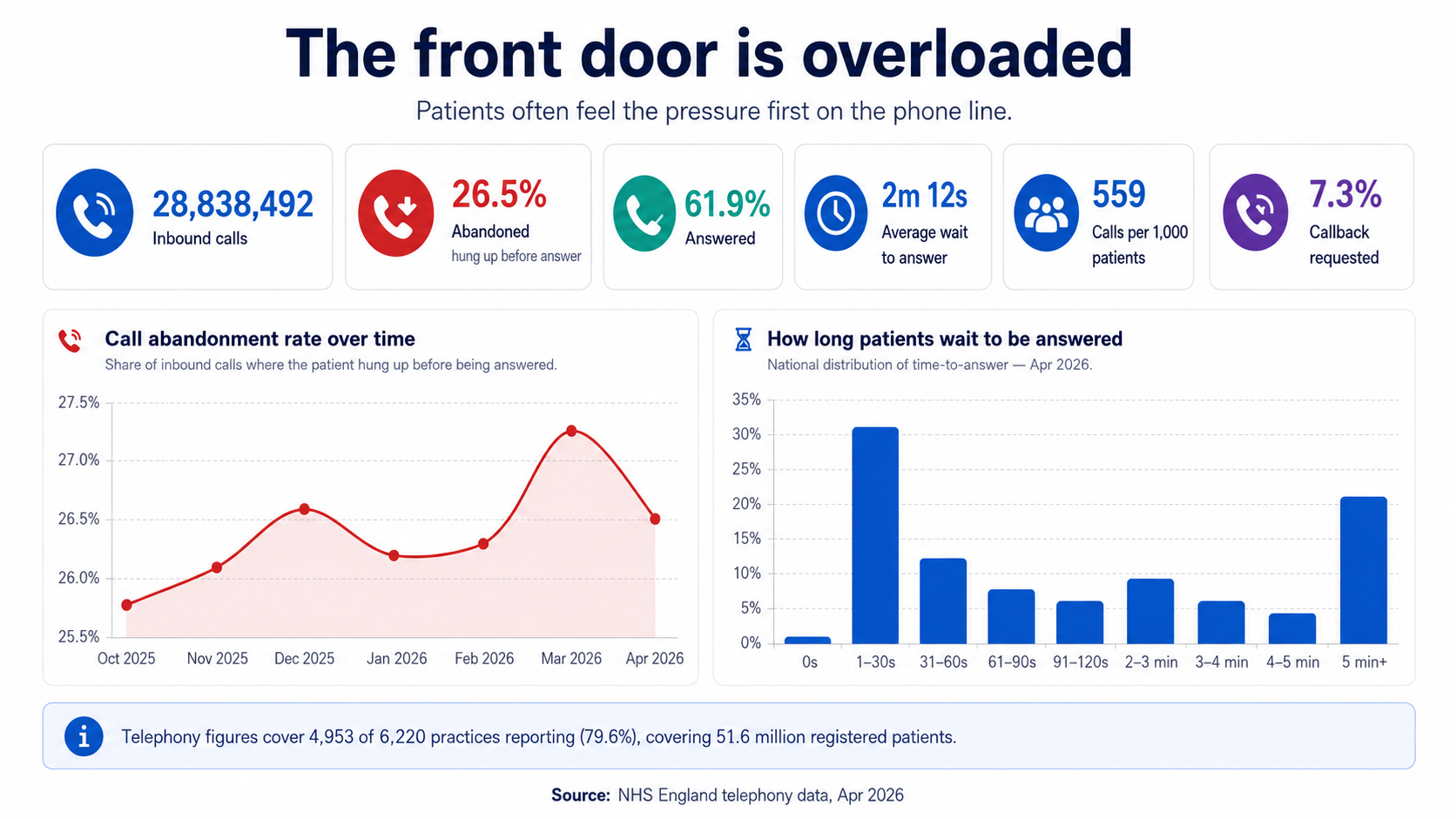
The available national telephony data for April 2026 recorded 28,838,492 incoming calls from the practices submitting data. Of those calls:
- Calls answered 61.9%
- Calls abandoned before answer 26.5%
- Average wait before answer 2 minutes 12 seconds
- Calls per 1,000 registered patients 559
- Calls requesting a callback 7.3%
These figures cover 4,953 of 6,220 practices, representing 79.6% of practices and approximately 51.6 million registered patients.2 They should therefore be interpreted with the reporting coverage in mind.
Abandoned calls do not all represent separate patients who received no help. Some callers redial, use a callback option, submit an online request or make contact through another route. Nevertheless, the figure clearly shows the level of frustration and repeated effort generated when demand reaches practices faster than teams can process it.
Now follow the money
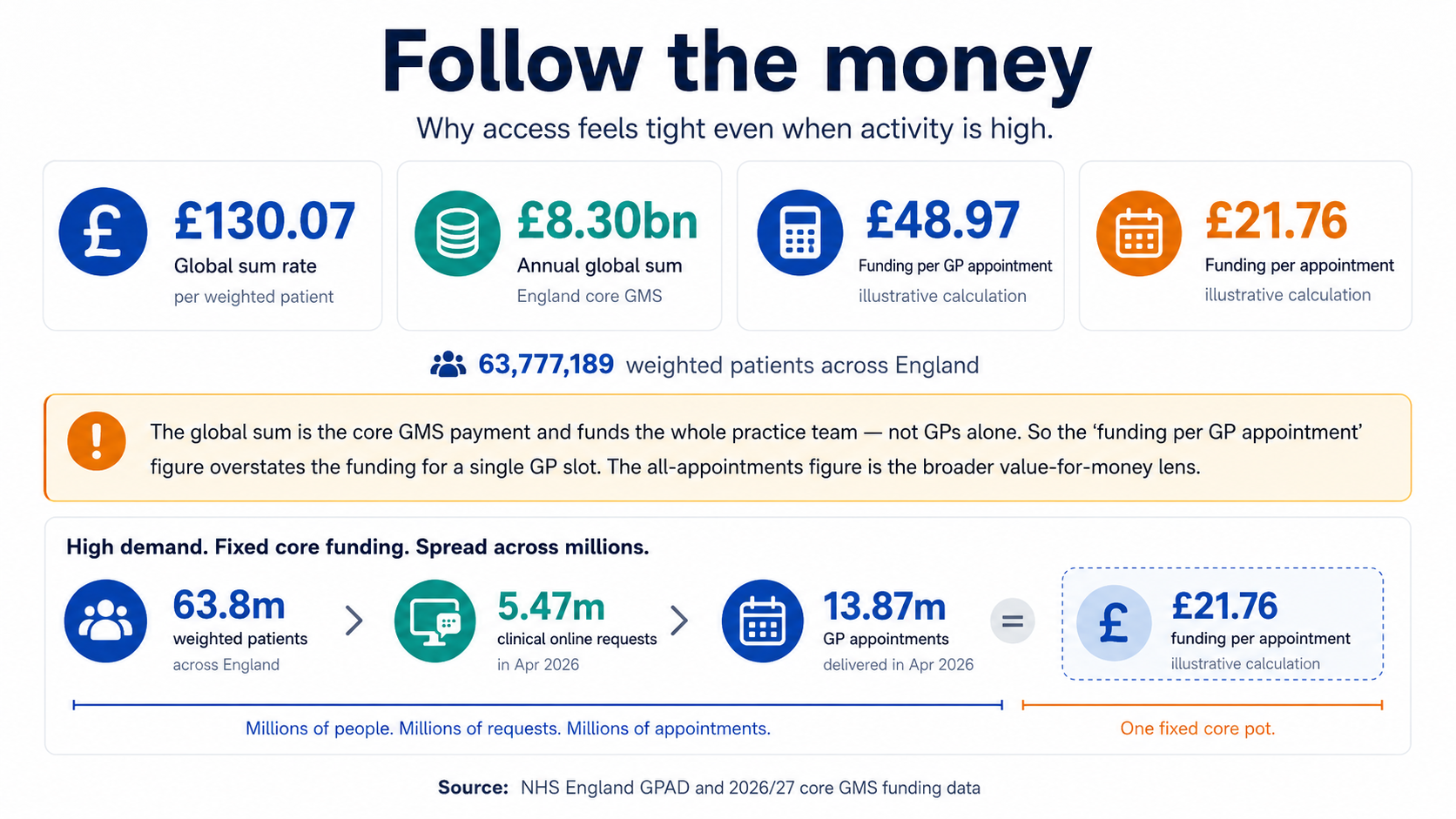
The core General Medical Services global sum for 2026/27 is £130.07 per weighted patient.3 The word weighted matters: practices are not simply paid £130.07 for every person on their registered list. The Carr-Hill formula adjusts practice populations to reflect factors including age, sex, morbidity, list turnover and local costs.
Applied to approximately 63,777,189 weighted patients across England, the global-sum rate produces an illustrative annual total of about £8.30 billion.
That sounds substantial—and it is—but it funds considerably more than a supply of GP appointments.
- GPs, nurses and healthcare assistants
- Reception, administration and management teams
- Premises and facilities
- Clinical systems and telecommunications
- Indemnity, insurance and professional costs
- Equipment, utilities and consumables
- Regulation, governance and mandatory compliance
- Results, prescriptions, referrals and non-contact work
- A payment made for each GP consultation
- A ring-fenced budget for appointment slots
- The salary of an individual GP
- A measure of practice profit
- The full value of every income stream received by practices
- A guarantee that funded capacity rises with daily demand
The global sum is the core contractual payment. Practices may receive additional income through the Quality and Outcomes Framework, Primary Care Network arrangements, enhanced services, premises reimbursements and other schemes. However, much of that funding is conditional, specified or tied to additional activity. It cannot automatically be treated as spare money available to create routine GP appointments.
What does the core funding look like against activity?
Dividing the estimated annual global sum by the latest trailing 12 months of GP-delivered appointments produces an illustrative figure of approximately £48.97 per GP appointment.
Dividing it by all recorded general-practice appointments produces an illustrative figure of approximately £21.76 per appointment.
These are comparisons, not payment rates
A practice is not paid £48.97 whenever a GP sees a patient, nor £21.76 whenever any appointment takes place. The calculation spreads the core global-sum pot across recorded activity to illustrate the scale of the funding available. Because the global sum also funds the infrastructure and wider team, the amount available for the consultation itself is necessarily lower.
The comparison also excludes significant work that is not always represented as a conventional appointment: reviewing results, issuing prescriptions, processing hospital correspondence, safeguarding work, referrals, reports, clinical supervision, care-home coordination and responding to online requests.
That is the structural issue. General practice is funded predominantly through population-based contractual arrangements, while demand arrives as an uncapped stream of calls, forms, messages, appointments and clinical risk.
Why access can feel worse even when more work is being done
Access is experienced individually. A national increase of several million appointments offers little comfort to somebody who cannot secure the particular appointment they need at their own practice.
Both of these statements can therefore be true:
General practice is delivering more activity
National datasets show sustained appointment volumes and rapidly growing online demand.
Patients can still struggle to obtain care
Demand can exceed the available capacity for particular clinicians, times, locations and types of appointment.
The contradiction disappears once we distinguish total activity from available capacity. A practice can be busier than ever and still have no safe additional appointments to release.
More contacts can also generate more follow-up work. An online request may lead to a telephone assessment, a face-to-face appointment, blood tests, a prescription and a referral. Counting only the eventual appointment misses the chain of work that produced it.
Capacity is also physical
Workforce is only one constraint. A clinician cannot hold a confidential consultation without a suitable room, functioning equipment and the administrative infrastructure around them.
Lord Darzi’s 2024 investigation reported that 20% of the primary care estate predates the foundation of the NHS in 1948.4
Practices may therefore be asked to expand teams and deliver more care from buildings that were never designed for modern multidisciplinary general practice. Recruiting another clinician does not create another consulting room.
What would improve access?
There is no single switch that will solve the problem. Sustainable access requires the different parts of the system to move together.
The real answer
Patients struggle to obtain GP appointments not because general practice has stopped delivering them, but because the service is absorbing more demand, through more channels, with finite staff, rooms and core funding.
Practices can redesign telephone queues, introduce online forms and make appointment books more efficient. Those changes matter. But efficiency cannot indefinitely compensate for a structural gap between what the service is expected to provide and the capacity available to provide it.
General practice does not have an appointment problem in isolation. It has a capacity, infrastructure and funding problem that patients experience as an appointment problem.
Methodology and important context
Appointment and online-request figures are drawn from NHS England’s published Appointments in General Practice data. Telephony figures reflect the practices reporting into the national telephony dataset and are not a complete census of every practice.
The annual global-sum and per-appointment figures are calculations produced by combining published population, contractual funding and activity data. They are intended to illustrate scale and should not be interpreted as actual payments made for individual appointments.
Figures may be revised in later NHS publications. Totals have been rounded where appropriate.